If you’re a general dentist looking to integrate dental aligners into your services, it’s essential to choose your first case carefully to ensure treatment success and patient satisfaction. Case selection is a crucial step, because allows you to start with cases of easy to medium difficulty, suitable for novice practitioners.
This article will guide you through the essential criteria for identifying the most appropriate cases to treat with French Aligners and help you know when it’s best to redirect more complex cases to an orthodontist.
Steps to follow when choosing your first case of dental aligners
To select the right cases for treatment, it’s important to follow a precise protocol. Here are the key steps in a clinical examination, which will help you to assess the complexity of a case. Il est toutefois crucial de comprendre que cette évaluation repose sur une analyse combinée de plusieurs facteurs, dont nous parlerons en détail ci-dessous.
If you have any questions about the complexity of a case, our clinical experts are on hand to provide support.
➡️Our teams can help you integrate aligners into your practice!
1. Clinical examination
The clinical examination in orthodontics is different from that in general dentistry.
In invisible orthodontics, particular attention is paid to the following aspects:
– Anterior and posterior occlusion ;
– Oral functions ;
– Temporomandibular joints;
– History of orthodontic treatment;
– Periodontal status;
– Any respiratory problems.

Occlusion assessment
It is essential to determine the molar and canine angle class during the clinical examination:
- Class II is characterized by the distal position of mandibular teeth in relation to maxillary teeth.
- Class III is defined by a very mesial position of the mandibular teeth in relation to the maxillary teeth.
It is also necessary to measure the overjet and overbite to select cases:
- The overjet is the horizontal distance measured from the free edge of the upper incisors to the free edge of the lower incisors in the anterior-posterior direction.
- The overbite is the vertical overlap measured by projecting the free edge of the upper incisors onto the vestibular surface of the lower incisors.
Cases with a Class II greater than 2 mm associated with an overjet greater than 4 mm should be referred to an orthodontist.
Examination of functions
Functional examination includes assessment of swallowing, chewing and breathing:
- Swallowing is considered dysfunctional if an anterior lingual interposition replaces the lingual tip that should rest on the palate during swallowing.
- Breathing should be nasal; buccal or mixed breathing may indicate a transverse deficit skeletal problem.
When dysfunction is associated with endognathy (a maxilla smaller than the mandible), the case should be referred to an orthodontist.
Identifying joint problems
Joint problems need to be identified, as they are often associated with occlusal problems, particularly in Class II or overbite cases. These cases require referral to an orthodontist.
Study of orthodontic treatment history
A history of orthodontic treatment should be taken into account, as some previous treatments can cause root resorption, which may contraindicate further orthodontic treatment.
Checking periodontal status
Periodontal condition influences the treatment plan. For example, in the case of generalized periodontitis, it is preferable to first stabilize the condition before considering orthodontic treatment. If the periodontitis is localized, it is essential to specify in the prescription not to move teeth affected by periodontal failure.
2. Assessment of dento-maxillary disharmony
Dento-maxillary disharmony (DMD) refers to the difference difference between the size of the jaw and the sum of the mesio-distal diameters of the teeth.
When this difference is positive, we speak of diastemas. Conversely, when the difference is negative, we speak of dental crowding.
For cases presenting dental crowding, it is crucial to quantify the latter in order to determine whether treatment can be carried out in-house or whether it is necessary to refer the case to an orthodontist. Anterior crowding is measured from the distal surface of one canine to the distal surface of the contralateral canine:
- Dimensions less than or equal to 6 mm This case is considered easy to moderate, depending on the extent of crowding and associated malposition. It can generally be treated without tooth extractions, using conventional methods to create space, such as premolar-molar expansion, incisal vestibulo-version, and interproximal reduction.
- Clearance greater than 6 mm : This case is considered difficult, often requiring tooth extractions to resolve the crowding problem. In these complex situations, especially when treating with aligners, referral to an orthodontist is recommended.
3. Classification of malocclusions according to the three spatial dimensions
To assess the difficulty of a case, it is useful to classify malocclusions according to the three spatial dimensions (see table below):
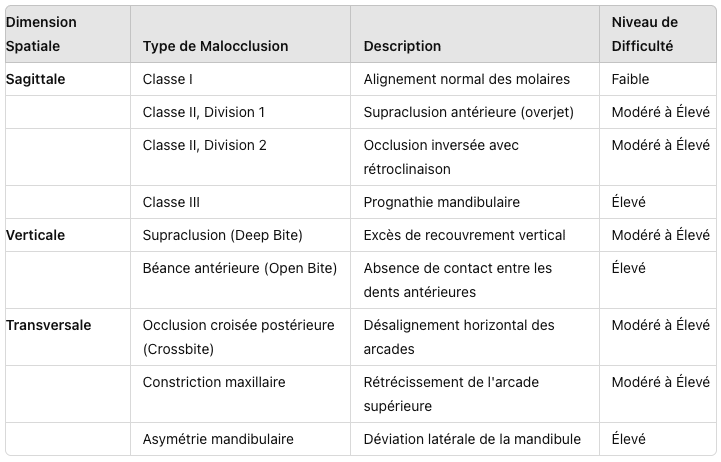
Anteroposterior dimension
- Class II: This malocclusion may be dental, skeletal or a combination of both. Cases with a Class II greater than 2 mm and an overjet greater than 4 mm should be referred to an orthodontist.
- Class III: Characterized by an overhang greater than 2 mm with a negative overjet. These cases should also be referred to an orthodontist.
Vertical dimension at alveolar level
- Overbite: Manifested by an excess of vertical overlap. Cases where the overlap exceeds 4 mm should be referred to an orthodontist.
- Infraclusion: Characterized by a lack of vertical overlap, with an overbite of between 0 and 2 mm.
- Open bite: When the overbite is negative. Cases with an overbite of less than -1 mm should also be referred to an orthodontist.
Transverse dimension
- Facial hyperdivergence: An increase in the lower level of the face.
- Facial hypodivergence: results in a reduction of this floor.
- Maxillary endognathy: The maxilla is reduced in size or has a lingual orientation of the maxillary alveoli.
- Maxillary exognathy: The maxilla is oversized or the maxillary alveoli are oriented too far vestibularly.
Skeletal problems such as endognathism or exognathism require consultation with an orthodontist.
4. Malpositions and tooth movements
Once malocclusions have been identified, it’s crucial to address the malpositioned teeth and the orthodontic movements required.
The complexity of the case increases in proportion to the number of teeth to be moved and the difficulty of the movements required. Treatments become more unpredictable and complex when they involve root or vertical movements, particularly for mandibular or multi-radiculate teeth. It is therefore essential to assess the complexity of tooth movements to determine whether treatment with aligners is viable.
To conclude
Choosing the right cases for treatment with dental aligners is essential toensure optimal results and boost your confidence as a practitioner. By assessing malocclusions along anteroposterior, vertical and transverse dimensions, you can select suitable cases for effective treatment.
For successful results, focus on easy to moderate cases. For more complex cases, we offer free training courses to help you deal with more difficult situations.